|
Welcome to a VIA Online Learning Tutorial: This site has been developed to provide learning materials to assist you to make complete and comprehensive radiographic examinations of animals.
Select Chapter:
1. BARIUM MEAL
2. ADDITIONAL GIT STUDIES
3. EXCRETORY UROGRAPHY
4. LOWER URINARY TRACT [print this page]

Retrograde cystography:
Both negative and positive contrast cystography will enable the bladder wall, mucosal margin and lumen to be visualised.
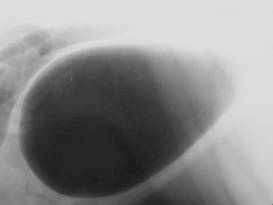
For negative contrast cystography, simply catheterise the bladder (using sterile technique), drain all the urine from the bladder and through a three way stop cock, instil air or gas into the bladder until it becomes slightly turgid (judged by palpation of the bladder through the abdominal wall). Take lateral and ventrodorsal radiographs.
 a a  b b
Fig 1: Normal pneumocystograpm, enabling the bladder wall, mucosal margin and lumen to be visualised.
 a a 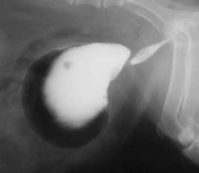 b b
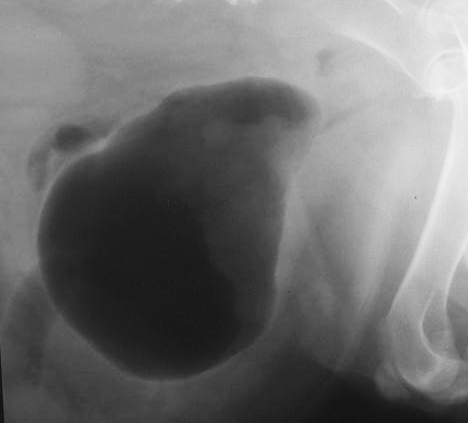
Figs 2: Negative [a] and double contrast [b] images of the bladder, demonstrating a mass infiltrating the ventral bladder wall.
Positive contrast cystography.
An extension of pneumocystography is to drain the air out of the bladder and replace it with approximately 50mL of positive contrast medium. Because positive contrast media can be expensive, and in large volumes can be excessively opaque, dilute it 50% with sterile water. The resulting diluted opacity doesn't diminish the radiographic detail of the bladder wall but does save cost while providing adequate visualisation of the bladder wall and intraluminal lesions. This positive contrast cystogram will show more acute detail of the mucosa and the bladder wall than is sometimes seen on a negative contrast study.
 a a 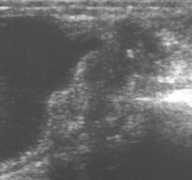 b b
Fig 3: Continuation of fig 8-3. In [a] is a pneumocystogram after evacuating as much positive contrast material as possible to demonstrate the mucosal margin of the mass. In [b] the mass is visualised using ultrasonography.
Double contrast cystography.
The third contrast procedure that you can perform is to then drain the positive contrast from the bladder and re-instil air until the bladder is again turgid. The radiographs you now take will reveal a double contrast study of the bladder. Any positive contrast which adheres to the mucosa of the bladder will usually do so because of inflammatory bladder wall lesions. This study will also help to identify small calculi which were previously not visible on the negative or positive contrast studies. Polyps, bladder wall infiltrating masses, urachal diverticuli and inflammatory bladder wall thickenings will all be identified using this sequence of bladder studies.
The dangers of negative contrast radiography of the bladder are small, but occasionally air embolisaton may occur, particularly if the patient has severe cystitis. If air embolisation occurs, or if iatrogenic gas dissection within the bladder wall is recognised, place the patient in left lateral recumbency. By placing the right cardiac chambers on the non-dependent side of the thorax movement of intravascular gas/air through the right heart will be hindered, buying time for it to be diluted and absorbed.
To avoid air embolisation, you can use either carbon dioxide or nitrous oxide instead of air. Both have high solubility in body fluids, and if they inadvertently enter the patient's blood will not cause problems due to air embolisation.
Retrograde urethro-cystography.
This study can be done in males or females. To provide effective retro-filling of the urethra, a small balloon tipped Foley catheter may be preferred instead of standard urethral catheter. The catheter is placed with its tip in the distal urethra and the balloon filled. The radiograph is exposed during the injection of contrast medium. In males, retrograde injection of positive contrast material into the urethra produces opacification of the membranous penile and the prostatic parts of the urethra as well as of the bladder neck.
 a a  b b
Fig 4: [a] Normal retrograde urethro-cystogram in a dog. The penile urethra [PU], membranous urethra [MU], prostatic urethra [Pr U], prostate [Pr] and urinary bladder [UB] are labeled. The catheter tip [arrow] is within the penile urethra. In [b] there is reflux of contrast into the prostatic ducts.
An undiluted injection of organic iodine contrast medium is used as the contrast material. For a simple urethrogram, preload the urethral catheter with contrast medium [to eliminate air bubbles] and inject 20mL of positive contrast material via the urethral catheter as quickly as possible, and have the radiograph exposed whilst injecting the last few mL's. The procedure should be repeated to enable lateral and an oblique ventrodorsal view to be taken. These views will demonstrate the urethral lumen and mucosal interface extending from the tip of the catheter to the bladder. The purpose of these studies is to evaluate the mucosa of the urethra in suspected cases of urethral neoplasia and to evaluate the urethra for evidence of compression or stenosis. A variation of this study is to precede the urethrogram phase by filling the bladder with either positive contrast material or saline so that it is turgid. The subsequent retrograde injection of the contrast material into the urethra should then maximally distend the prostatic urethra. This second variation of the urethral study is useful in those instances where the first urethral study does not adequately distend the prostatic urethra.
Retrograde vagino-urethro-cystography.
This study is achieved by filling the vagina with positive contrast media. By overfilling the vagina, contrast medium retrofils the urethra. The study requires the labia to be occluded to enable adequate dilation and opacification of the urethra. Because urethral distension is momentary, the radiograph is taken during active filling of the vagina and urethra.
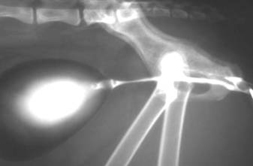
Fig 5: Normal female urethra in a cat, obtained by retrograde vagino-urethrography.

Fig 6: Retrograde vaginourethrogram to demonstrate bilateral ectopic ureters in a dog. The vestibule [Ve], vagina [Va] and urethra [U] are visible caudal to the urinary bladder [UB]. The right and left ureters [R and L] enter the urethra [arrows.
<< Previous chapter "Excretory Urography"
|